 Elbasvir-Grazoprevir Zepatier
Elbasvir-Grazoprevir Zepatier Glecaprevir-Pibrentasvir Mavyret
Glecaprevir-Pibrentasvir Mavyret Ledipasvir-Sofosbuvir Harvoni
Ledipasvir-Sofosbuvir Harvoni Ribavirin Copegus, Rebetol, Ribasphere
Ribavirin Copegus, Rebetol, Ribasphere Sofosbuvir Sovaldi
Sofosbuvir Sovaldi Sofosbuvir-Velpatasvir Epclusa
Sofosbuvir-Velpatasvir Epclusa Sofosbuvir-Velpatasvir-Voxilaprevir Vosevi
Sofosbuvir-Velpatasvir-Voxilaprevir VoseviOverview
There are an estimated 4.1 million Americans infected with hepatitis C virus (HCV) infection, making hepatitis C the most common blood-borne infectious disease in the United States.[1] It is also associated with significant morbidity and mortality, driven largely by progression to liver cirrhosis, liver cancer and death. Hepatitis C infection is often associated with substance use, mental health disorders and poverty, all of which contribute to the stigma and discrimination associated with this infection. Since 2014, hepatitis C has become one of the few chronic viral infections that can be cured through the use of safe, well-tolerated, oral direct-acting antiviral (DAA) medications. Current recommended DAA therapy cures HCV infection in 95% or greater of treated persons.[2] The availability of DAA therapy has revolutionized the management of hepatitis C and provides an opportunity not only to prevent the negative health consequences of hepatitis C at the individual level but also to prevent new infections by reducing the reservoir of people infected with HCV who can, in turn, transmit HCV to others. This concept of treatment as prevention is supported by modeling data and more recent real-world data suggesting that treating a significant proportion of people infected with hepatitis C can over time lead to reductions in both incident and prevalent infections over time.[3,4,5]
CDC 2025 and 2030 HCV Elimination Goals
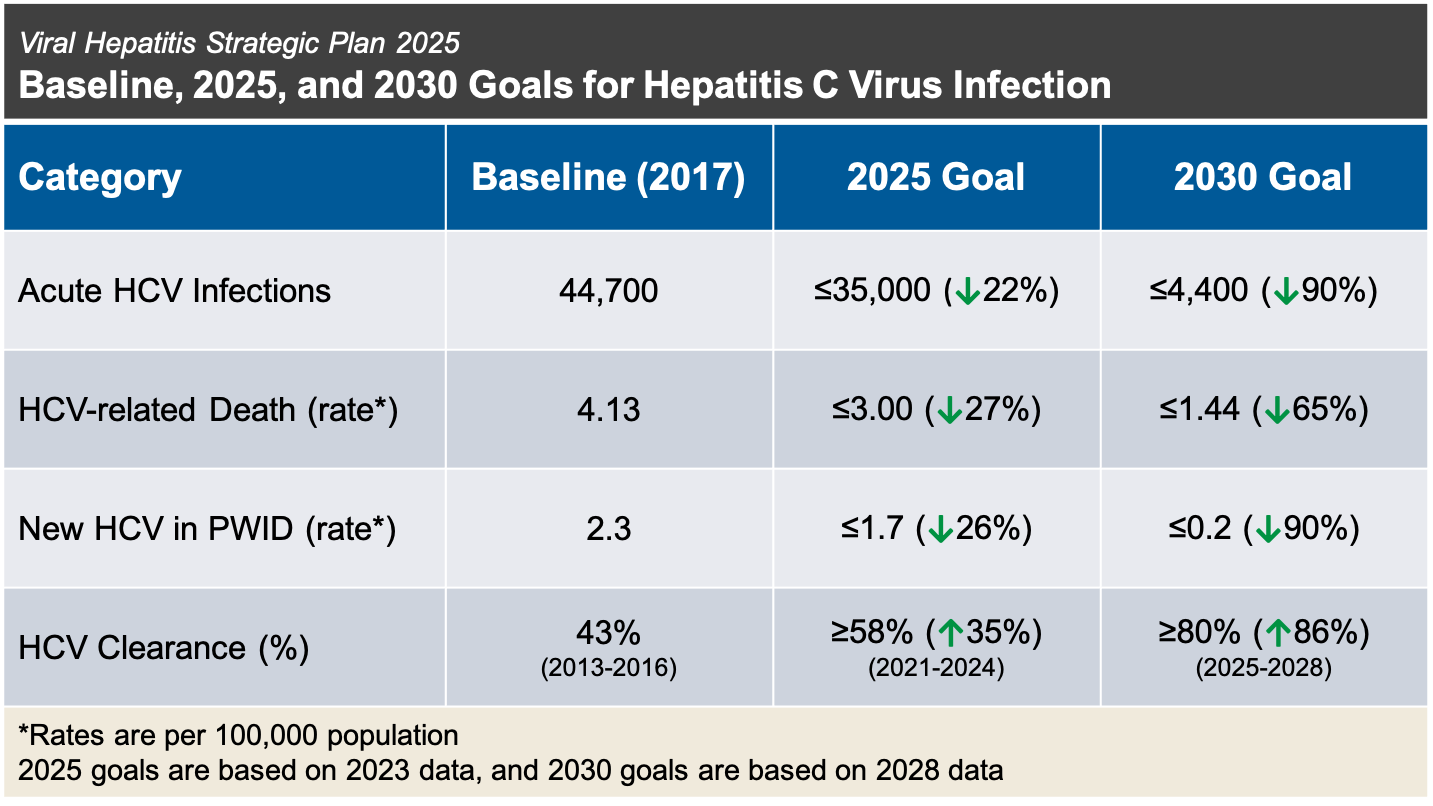
The Division of Viral Hepatitis at the Centers for Disease Control and Prevention has issued a 2025 strategic plan for HCV elimination that outlines the following goals for 2025 and 2030 when compared to a baseline in 2017 (Figure 1).[6]
- Decrease new HCV infections by 20% for 2025 and by 90% for 2030
- Reduce HCV-related death rate by 25% for 2025 and by 65% for 2030
- Reduce rate of new HCV infections in persons who inject drugs by 25% for 2025 and by 90% for 2030
- Increase proportion of persons with HCV viral clearance by 35% for 2025 and by 85% for 2030
These HCV elimination goals have proved challenging in the midst of the ongoing opioid epidemic in the United States.[7,8,9] Indeed, in 2019, there was a 70% increase in incident HCV infection compared to new infections in 2015.[11] Multilevel barriers at the patient, provider, and system levels contribute to difficulties with access to HCV testing and treatment, substance use treatment and harm reduction services required to achieve HCV elimination goals. This topic review will identify and discuss the major structural barriers to HCV treatment in the United States.